
Blue light, is also known as high-energy visible (HEV) light and is the most energetic part of the visible light spectrum (380 - 700 nm) with wavelengths ranging from indigo or ultramarine light 420-440 nanometers, blue light 450-495 nanometers to cyan light 480 - 520 nanometers. Blue light has lower energy than ultraviolet (UV) radiation (280–400 nm) and can reach further into the dermis, up to the depth of 1 mm. [1] Sunlight is the primary natural source of blue light. Up to 50% of the damaging oxidative stress in human skin is generated in the VIS spectrum and the other 50% by UV light [2], contributing to premature ageing, ox-inflammageing and hyperpigmentation like age spots.
Blue light from electronic devices The use of electronic devices has led to increased exposure to artificial blue light sources, however the amount of blue light emitted during the conventional use of electronic devices is by far not enough to trigger harmful skin effects. If you sit in front of a monitor uninterrupted for a week at a distance from the screen of approximately 30 cm, this would be the same as the blue light intensity of spending one minute outside on a sunny day in Hamburg Germany at around midday at midsummer. If you hold a smartphone right next to the skin, the intensity does increase, but it would still take approximately 10 hours of uninterrupted use to match the effect on the skin of just one minute of sunlight. The emissions from electronic devices are barely noticeable in comparison to natural blue light directly from the sun and are, thus negligible. However, blue light or HEV light from sunlight can be harmful for skin. Dr Ludger Kolbe Chief Scientist for Photobiology and his team at Beiersdorf AG did pioneering research regarding the harmful effects of HEVIS. [3-4] I would also like to take the opportunity to debunk an important myth at the start of this article as infrared or near infrared light does not induce damaging free radicals (even in high amounts), there is no such thing "infra-ageing" as a result or IR and in fact red light photobiomodulation supports skin rejuvenation. Read more Direct effects of blue light and HEV Light on skin Blue light and HEV light can have both beneficial and detrimental effects on the skin. The most significant direct effects are mediated through their interaction with chromophores, such as flavins, porphyrins, and opsins, which can trigger the overproduction of reactive oxygen species (ROS), reactive nitrogen species (RNS). and hyperpigmentation. Reactive oxygen and nitrogen species cause DNA damage and modulate the immune response. [1] This oxidative stress can lead to: Photo-ageing: Exposure to blue light and HEV light can induce premature skin aging, causing wrinkles, fine lines, and loss of elasticity. Hyperpigmentation: Blue light and HEV light can stimulate melanin production, leading to uneven skin tone and the development of age spots or other forms of hyperpigmentation. DNA Damage: The ROS and RNS generated by blue light and HEV light can cause DNA damage, plus potentially increase the risk of skin cancer. Inflammation: The oxidative stress triggered by blue light and HEV light can cause an inflammatory response in the skin, exacerbating conditions like acne, eczema, and psoriasis. Molecular and physiological mechanisms of direct blue light effects on the skin [1]
Indirect effects of blue light and HEV Light on skin Blue light and HEV light can also have indirect effects on the skin by disrupting the body's circadian rhythms. This occurs via both the central mechanism, which involves stimulation of light-sensing receptors located in the retina, and via the peripheral mechanism, which involves direct interaction with skin cells. By disrupting the normal circadian rhythm, blue light can negatively affect the skin's natural overnight repair and regeneration processes. [1] The circadian rhythm has been shown to affect multiple cellular and physiological processes occurring in the skin:
Molecular mechanisms of indirect effects of blue light on the skin [1]
Ideal daytime & nighttime skin care regimen When considering cosmetic interventions, a strategy of daytime protection plus defense and night-time repair may be optimal. The skin's own repair mechanisms, such as base excision repair and nucleotide excision repair, attempt to mitigate blue light induced DNA damage. [12] Daytime protection plus defense Of course prevention and/or reduction of blue light exposure from sunlight is key. Reduce the time spent on electronic devices, especially before bedtime, can help minimize the disruption of circadian rhythms and the indirect effects of blue light and HEV light on the skin. Against premature ageing and hyperpigmentation an evidence based effective approach could be the daily use of tinted broadband sunscreen preferably containing Licochalcone A (the most effective anti-oxidant reducing damaging free radical activity from both UV and blue light and moreover protects against collagenase MMP-1 expression) strengthening skin's biological defense [4-5-6-7], while iron oxides in colour pigments provide physical protection against blue light (like zinc oxide and titanium dioxide). Against hyperpigmentation there are (tinted) sunscreens which on top contain the most potent human tyrosinase inhibitor found in dermatological skin care called Thiamidol® [8-9] and one of the 3 ingredients in the "new Kligman Trio" (NT) [18] and Glycyrrhetinic Acid which supports skin's DNA repair and skin pigmentation [10] and inhibits hyaluronidase activity (HYAL1). Most regular sun filters used in sunscreen don't offer any protection against blue light, however according to the website of BASF the chemical UV filters Tinosorb® A2B and Tinosorb® M can reduce the exposure to blue light. [11] Scattering and absorption of blue light [5] The penetration depth of visible light is influenced by the reflection, scattering, and absorption mediated not only by the skin’s physical barrier but also by the VL chromophores in the skin and Fitzpatrick skin or photo-type (FST). The primary VL-scatter and absorption molecules in the skin include hemoglobin, melanin, bilirubin, carotene, lipids, and other structures, including cell nuclei and filamentous proteins like keratin and collagen. Melanin and keratins are the primary VL absorbers and scatterers in the epidermis, while hemoglobin is the dominant absorber, and collagen is the major VL scatter in the dermis. Melanin's absorption spectrum ranges from 200 to 900 nm, with the peak absorption varying based on melanin moiety.. This means that individuals with darker skin types, which have higher melanin content, are more prone to hyperpigmentation from blue light or VIS due to the greater absorption and scattering of VIS in their skin on top of the previously mentioned higher levels of tyrosinase–DCT complexes leading to increased melanogenesis, leading to both transient and long-lasting pigmentation [13], dependent upon the total dose and exacerbation of melasma especially in individuals with FSTs III to VI. Blue light tanning Recent data demonstrate synergistic effects between VL and UV-A on erythema and pigmentation. VL-induced pigmentation is more potent and more sustained than UVA1-induced pigmentation in darker skin tones.Typically, three mechanisms are involved in the responsive reaction of melanocytes to VL, with increased melanin content: immediate pigment darkening (IPD), persistent pigment darkening (PPD), and delayed tanning (DT). [15] Read more. VL can also exacerbate post inflammatory hyperpigmentation (study with FST IV and V). [16] Blue light therapy While the detrimental effects of blue light and HEV light on the skin have been well-documented, these wavelengths have also shown promise in the treatment of certain skin conditions. In controlled clinical settings, blue light has been used to: Treat Acne: Blue light can reduce the growth of Propionibacterium acnes, the bacteria responsible for acne, and has an anti-inflammatory effect. Manage Psoriasis and Atopic Dermatitis: Blue light has been found to have an anti-inflammatory and antiproliferative effect, making it potentially beneficial for the treatment of these chronic inflammatory skin diseases. Reduce Itch: Some studies have suggested that blue light may help alleviate the severity of itching in certain skin conditions. The optimal protocols for blue light therapy are still being developed, and the long-term safety of this treatment modality requires further investigation and should not be initiated without HCP recommendation and monitoring. Vitiligo: Blue light therapy via LEDs can stimulate repigmentation in patients with vitiligo with minimal adverse events, however larger studies are needed. [17] Overall, the research suggests that prolonged or excessive exposure to high-energy blue light, can have negative long-term effects on skin structure, function, and appearance in all phototypes. As our understanding of the individual variations in skin's response to blue light exposure deepens, the development of personalised or tailored effective solutions become increasingly more tangible. Always consult a qualified healthcare professional or dermatologist to determine what the most suitable approach is for your particular skin condition and rejuvenation goals. Take care! Anne-Marie References
Comments

If you've scrolled through Instagram, you may have caught a glimpse of dermatologists raving about LED masks emitting red light, the secret, evidenced based weapon behind skin rejuvenation known as photo biomodulation. It uses low-powered light within the red to near-infrared range (wavelengths from 632 to 1064 nm) to induce a biological reaction aka stimulate cellular processes. The wonders of red light, also known as LLLT (low-level laser therapy), PBM (red light photo-biomodulation), or PBMT (photo-biomodulating therapy), extend far beyond non-invasive skin rejuvenation. I am not a fan of devices for home use, mostly because of lacking safety and/or efficacy, PBM definitely earned it's prominent spot in my skincare routine.
A summary of the benefts of red light with and without near infrared light for skin Numerous studies have demonstrated the effectiveness of red and infrared light therapy for skin rejuvenation. A combination of red light and near IR light has proven to stimulate the production of collagen (I & III) plus elastin production (Li WH et al Int J Cosmet Sci 2021), enhance mitochondrial ATP production, cell signaling, growth factor synthesis, rebalance ROS (reactive oxidative species) and reduce inflammation. Stem cells can be activated allowing tissue repair and healing. Wrinkle and scar reduction was observed and it can reduce UV damage both as treatment and prophylactic measure. In pigmentary disorders such as vitiligo, it can increase pigmentation by melanocyte proliferation and reduce depigmentation by inhibiting autoimmunity (Pinar Avci et al. Semin Cutan Med Surg. 2013 & Mitchell J Winkie et al. Review Photodermatol Photoimmunol Photomed A focused review of visible light therapies for vitiligo 2024). It has the potential to activate both keratinocytes (epidermis) and fibroblasts (epidermal junction and dermis). With consistent use, you can expect a reduction of lines and wrinkles, improvement of skin tone and texture. PBMT (when done effective and safe) will compliment both your skin rejuvenating and regenerating at home skincare regimen and in-office procedures or even post-surgical skin recovery. ATP ATP (adenosine triphosphate) is the primary source of energy for cellular processes and plays a crucial role in various biological functions. When red light with specific wavelengths (630 nm to 638 nm and 810 nm) is absorbed by the skin cells, it stimulates the mitochondria, which are the powerhouses of the cells responsible for ATP synthesis. This increase in ATP production is providing cells with more energy to carry out their functions effectively and has several beneficial effects on the skin like boosting cellular metabolism, promoting more efficient nutrient uptake and waste removal. The increased ATP levels facilitate collagen synthesis by fibroblasts, a vital component for skin structure, elasticity and firmness and reduction of lines and wrinkles.. ATP aids in the repair and regeneration of damaged skin cells. It accelerates the healing process, making it beneficial for wound healing, post-surgical recovery, and addressing skin issues such as acne scars. ROS (Reactive Oxidative Species) By modulating ROS levels, red light therapy helps reduce oxidative stress and its detrimental effects on the skin. ROS are highly reactive molecules that are naturally produced by cells as byproducts of metabolic processes. While low levels of ROS play important roles in cellular signaling and immune responses, excessive ROS can lead to oxidative stress and damage to cells and tissues. Restoring the balance of ROS result in improved skin health, reduced inflammation, and enhanced skin rejuvenation. Red light therapy has been shown to modulate reactive oxidative species (ROS) levels in the skin by promoting antioxidant defense mechanisms and reducing oxidative stress:
The difference between LLLT and PBM LLLT refers specifically to the use of lasers, which produce coherent, focussed and an intense beam of monochromatic light, while PBM has a broader range of light sources, may include laser as well as light-emitting diodes (LEDs) and other non-laser devices. LEDs are often used in PBM because they are cost effective, versatile and have the ability to cover large treatment areas. LLT uses higher power densities with more energy and has a shorter treatment duration in comparison to PBM to achieve desired therapeutic effects. While there are similarities in terms of mode of action", there is a difference of light source, treatment application and parameters. Based on consensus, PBM and PBMT are considered the correct way to describe this photonic specialty for therapeutic applications. In this post I will focus on PBM and specifically LEDs. LED masks and LED panels LED masks specifically produced by the brand Omnilux (FDA cleared) are currently very popular for very good reasons; they are safe and effective when the LEDs emit the right wavelengths and used in the recommended frequency. Omnilux combines 2 therapeutically effective and complimentary wavelengths: 633nm and near-infrared 830 nm. Both wavelengths (more precise 630nm + 850nm) I would recommend to minimally look for in any red LED device, which will disqualify most LED masks and panels in the market! I've include some (not affiliated) links to devices below. Both masks and panels can be effective, however most panels are stronger in comparison to masks 60 mW/cm² vs mW/cm²), hence have the benefit of a shorter treatment time to get a similar result. Intensity and power of red light therapy devices are typically measured in terms of irradiance (measured in milliwatts per square centimeter, mW/cm²) and radiant flux (measured in watts, W), which quantify the amount of light energy emitted by the device. Wearing a mask during a hot summer or in a warmer climate will make you sweat and depending on the materials of the mask and straps, they may be very uncomfortable to wear. Panels have the benefit that they give a more even distribution of emitted light as masks are worn on the face and thus the LED bulbs are pushed on a small skin surface area, panels can cover a larger area (depending on their size) and are more versatile in use, as area's like neck, décolletage, or knees are easier to treat with a panel. With a mask you may be more mobile, although I would not recommend walking around while using the mask. My personal preference would be a panel for the reasons mentioned before and panels are more suitable (more hygienic) for family sharing. My son can use it after an intense workout to speed up his recovery and I like to use it for purposes beyond photo-biomodulation or skin rejuvenation, for example to improve my sleep. With a panel I get more "bang for my buck". 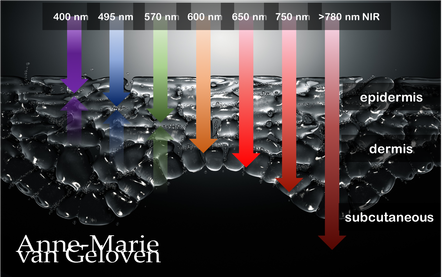
Red light and NIR (Near Infra Red light) have the ability to penetrate varying depths of the skin, resulting in distinct benefits, thus combinations of wavelengths will provide complementary effects.
630 nm Wavelength This wavelength is often used for its skin rejuvenation benefits. It has a relatively shallow penetration depth and is absorbed closer to the surface of the skin primarily affecting the epidermis. 630nm light is associated with increased circulation, reduce inflammation, improved skin tone & texture, aiding in the delivery of nutrients and oxygen to skin cells, and stimulating the production of collagen, leading to improved skin elasticity and a reduction of the appearance of fine lines & wrinkles. 660 nm Wavelength At 660nm, red light can penetrate a little deeper into the skin, reaching the dermis. It is known for its ability to stimulate collagen production, enhance cellular metabolism, and promote anti-inflammatory effects, helping to reduce redness and inflammageing. It also promotes wound healing, making it beneficial for post-surgical or post-trauma skin recovery. 810 nm Wavelength Improve healing & recovery & accelerate wound healing. 830 nm Wavelength Accelerate healing, reduce infection, improve aesthetic outcome following plastic surgery, increase endorfines (mood-enhancing), improve bone repair and growth. 850 nm Wavelength Improve general inflammation body, enhance muscle recovery, improve wound healing, reduced fine lines, wrinkles and hyperpigmentation. Always consult a qualified healthcare professional or dermatologist to determine if and what the most suitable red light therapy approach is for your particular skin condition and rejuvenation goals. Take care! References: Hamblin, Michael R. "Mechanisms and applications of the anti-inflammatory effects of photobiomodulation." AIMS biophysics 4.3 (2017): 337-361. Barolet, Daniel. Regulation of Skin Collagen Metabolism In Vitro Using a Pulsed 660 nm LED Light Source: Clinical Correlation with a Single-Blinded August 2009Journal of Investigative Dermatology 129(12):2751-9 Wunsch A, Matuschka K. (2014). A controlled trial to determine the efficacy of red and near-infrared light treatment in patient satisfaction, reduction of fine lines, wrinkles, skin roughness, and intradermal collagen density increase. Journal of Cosmetic and Laser Therapy, 16(5), 232-237. Avci P, et al. (2013). Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Seminars in Cutaneous Medicine and Surgery, 32(1), 41-52. Links to some devices which combine 630 nm and 850 nm: FDA-approved devices ensure safety and regulatory compliance, however the panels are more powerful: Omnilux(tm) Mask (FDA clearance) Very affordable panel (no FDA clearance) Affordable panel (no FDA clearance) 
Glycation is one of the basic root causes of endogeneous (intrinsic) skin ageing and a very challenging one or almost impossible one to reverse. Glycation is an ageing reaction which begins in early life, developing clinical symptoms at around 30, and progressively accumulates in tissues and skin due to the glycated collagens that are difficult to be decomposed. Glycation occurs naturally in the body when sugars react with proteins and lipids to form advanced glycation end products (AGEs). AGEs can be exogenously ingested (through food consumption), inhaled via tobacco or endogenously produced and formed both intracellularly and extracellularly. AGE modifications lead to dermal stiffening, diminished contractile capacity of dermal fibroblasts, lack of elasticity in the connective tissues, contribute to hyperpigmentation and a yellowish skin appearance. The formation of AGEs is amplified through exogenous factors, e.g., ultraviolet radiation.
AGEs cause changes in the skin through 3 processes:
One study published in the Journal of Investigative Dermatology found that levels of AGEs were higher in the skin of older individuals compared to younger ones. The study also showed that there was a correlation between the level of AGEs and the severity of skin ageing. This suggests that inhibiting the production or accumulation of AGEs in the skin is a potential target for anti-ageing interventions or skin ageing management. AGEs are complex and heterogeneous, more than a dozen AGEs have been detected (however not all) in tissues and can be divided into three categories according to their biochemical properties. AGEs are formed through four pathways:
GLYCATION INHIBITION IS KEY AGEs can be crosslinked through side chains to form a substance of very high molecular weight, which is not easily degraded. The consequences from skin glycation are irreversible. This makes prevention or inhibition of the process the best potential strategy to maintain skin health and ageing skin management. One way to do this is by altering the diet to reduce the intake of sugars and carbohydrates, which are known to contribute to glycation. Several studies have found that reducing sugar intake can result in significant improvements in skin health, including reducing wrinkles and improving skin texture. 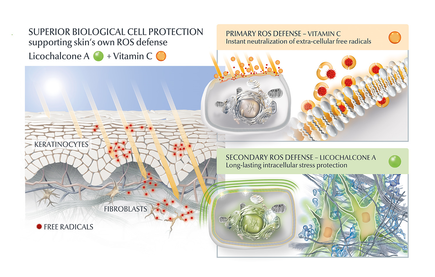
AGE inhibitors
Another potential strategy is the use of topical agents that inhibit the formation or accumulation of AGEs in the skin. One study published in the Journal of Cosmetic Science found that a cream containing carnosine, a peptide that inhibits glycation, improved skin elasticity and reduced the appearance of wrinkles in individuals with ageing skin. Skincare containing NAHP or Acetyl Hydroxyproline inhibits the formation of AGEs significantly (in vitro), most likely through a mechanism where NAHP competes with the proteins for the sugar. Finally, NAHP sacrifices itself in place of the proteins and gets (at least partially) glycated. NAHP also prevents loss of cellular contractile forces in a glycated in vitro dermis model and counteracts the diminished cell-matrix interaction that is caused by glyoxal-induced AGE formation. Anti-Oxidants Moreover, I would suggest to combine those ingredients with an ingredient like Licochalcone A. Numerous high ranked publications support that Licochalcone A protects cells from oxidative stress mediated by e.g. UV and HEVIS (blue light) induced reactive oxidative species (ROS). Due to the activation and nuclear translocation of the transcription factor NrF2, the expression of anti-inflammatory, antioxidant and detoxifying enzymes are induced. These enzymes protect the skin cells (like keratinocytes and fibroblasts) from ROS-induced damage, like lipid peroxidation and DNA as well as protein damage. If Licochalcone A is combined with L-Ascorbic Acid, (the most active form of Vitamin C), it supporting skin's own collagen production, provides superior biological cell protection amongst other relevant benefits. My absolute favourite product is Eucerin Hyaluron-Filler Vitamin C Booster which I use daily as a serum in my morning routine. GLYCATION AND SKIN HEALTH Acne In addition to its role in ageing, glycation in the skin has also been linked to a range of skin health problems. One study published in the Journal of Cosmetic Dermatology found that the level of AGEs in the skin was significantly higher in individuals with acne than in those without acne. The study also showed that treating acne with a topical antibiotic significantly reduced the levels of AGEs in the skin. Atopic Dermatitis Another study published in the Journal of Investigative Dermatology found that individuals with atopic dermatitis had higher levels of AGEs in their skin than healthy individuals. This suggests that glycation may play a role in the development of inflammatory skin conditions. Diabetes + Woundhealing The correlation between high sugar levels and skin ageing can be seen in diabetic patients, where one-third of this population has skin complications. A prominent feature of ageing human skin is the fragmentation of collagen fibers, which severely damages the structural integrity and mechanical properties of the skin. Elevated levels of MMP-1 and MMP-2 and higher crosslinked collagen in the dermis of diabetic skin lead to the accumulation of fragmented and crosslinked collagen, thereby impairing the structural integrity and mechanical properties of dermal collagen in diabetes. Collagen crosslinking makes it impossible for them to easily repair, resulting in reduced skin elasticity and wrinkles. Keratinocytes and fibroblasts are the main cells involved in wound healing, but due to the high glucose (HG) microenvironment in diabetics, the functional state of these cells is impaired, thereby accelerating cellular senescence (programmed cell death). Conclusion We can't completely stop the glycation process, therefore it's important that we inhibit it from a young age onwards, hence monitor the sugar intake of our children, use daily SPF and invest in good dermo-cosmetic products containing ingredients like NAHP and powerful anti-oxidants like L-Ascorbid Acid (Vitamin C is needed for the production of collagen) and Licochalcone A (also anti-inflammatory). Preventing signs of ageing, specifically caused by glycation is most effective. If your skin shows (advanced) signs of ageing, you can get visible improvement using skin component (hyaluron, collagen and elastin) bio-stimulating ingredients like Retinol, Bakuchiol, Arctiin, Creatine or Glycine Saponin. Consult your dermatologist if you wish to improve your skin's appearance or skin health issues. Take care Special thanks: Ph.D. dr Julia M. Weise Manager Biological Testing & Dorothea Schweiger Lab Manager Facial Skin Biology Beiersdorf HQ Hamburg 7/22/2018 Comments Chemical or mechanical exfoliation
We can support's skin natural exfoliation process in various ways, for example with mechanical or chemical exfoliation.
Desquamation (shedding of skin cells thus exfoliation) is an important part of the skin's natural regeneration or renewal process. Already in our twenties, this process slightly, however increasingly starts to slow down (Kligman 1983). As a result, the cells on the surface of our skin (corneocytes) become bigger (Kligman 1989) and a little disorganised. This leads to a duller appearance (loss of radiance) and a more rough texture of our skin. A very comprehensive comparison of both methods:
The word "acid" unfortunately sounds very harsh and skin-unfriendly. Many acids are actually skin's own, like for example lactic acid is a skin's own natural moisturising factor (NMF) and so is hyaluronic acid. The level of NMF's decrease as we age and our skin my lose the ability to maintain well hydrated. Many years ago the benefits of lactic acid were capitalised by using baths filled with donkey milk. Citric acid is commonly used in skin care products and toners to balance skin's pH. Gluconolactone is only gradually penetrates skin and is very gentle.
It's unfortunate that "acids" have such a negative connotation, as our skin (healthy and problematic) can benefit if we use them regularly. Moreover, I prefer this method over mechanical exfoliation for all skin types, however particularly if you have dry skin, acne- or redness prone skin, sensitive skin or mature skin. The risk of exfoliation is over-exfoliation. Over-exfoliation is damage of our skin barrier and the symptoms are very comparable to dry or (hyper) sensitive skin symptoms, which are: redness, irritation, tightness, excessive dryness, dry patches, flaking skin, uncomfortable stinging, or even burning sensation. Whenever you experience one or more symptoms of over-exfoliation, it's recommended to reduce the number of times you exfoliate and support the skin barrier repair with a moisturiser. Hope you enjoy healthy skin & take care. 
Understandably we want to get rid of pimples as soon as possible and sometimes apply harsh products to our skin in order to shrink them.
Depending on which ingredient is used, you might inflict injury to the skin and it's barrier which is very comparable to a mild burn. There is even a phenomenon called "toothpaste burn". During the healing process there is a risk of scarring. A study published by Tan J. et al in JJD 2017 shows that up to >87% of patients with mild to moderate acne reports atrophic scarring (sunken scar) to some degree. A healthy skin barrier and well hydrated skin will support a the healing process. However, as the barrier is impaired and the skin dried out, the skin's regeneration and healing process will take longer. Therefore be careful with "shrinking" pimples. The same applies for "popping" pimples, as this method by definition will cause injury to the skin. Picking and squeezing pimples will further irritate the skin tissue and delay proper healing. The risk of scarring is increased when the tissue is inflamed. A recent study of prevalence and risk factors of acne scarring confirmed that there is a relationship between the time between onset and effective treatment. Acne scars can be more difficult to treat than acne! It's better to seek expert advice if you have problematic skin. Take care. 7/12/2018 Comments Relation skin pH and ageing process
A high pH value contributes to premature ageing skin!
A study published in British Journal of Dermatology showed that women with an alkaline stratum corneum (outer layer of the skin) developed more fine lines and crow's-feet (wrinkles at the outside corner of the eyes) than those with acidic skin over an eight-year period. This might be in part because an alkaline epidermis (top layer of the skin) tends to be drier and more fragile than an acidic one. Irritants can enter the skin and water can evaporate more easily. People with hydrated skin showed a 50% lower rate of wrinkling than those with dry skin. If the acid mantle is not intact, it can make skin more susceptible to inflammation (inflammaging) and lowered enzymatic activity, which again increases the risk of development of signs of ageing. Last but not least, alkaline skin is more prone to sun damage thus photo-aging, because its protective barrier has been weakened. pH balance is fragile. I just mentioned that alkaline skin tends to be drier, however it’s also known that the oils secreted by our skin impact skin’s pH by increasing it. This is one of the reasons that oily skin types can be more prone to acne, as the skin’s pH influences it's microflora. That's a topic for another blog post. You’ve maybe seen some of my previous posts on skin’s pH and it’s actually one of my major topics. This is because healthy skin starts with an optimal pH balance. Click below in the featured categories on “Skin pH” if you like to learn more about pH. If there is a specific topic you are interested in missing, please place a comment below and I will see to it that I address it. Take care. 7/10/2018 Comments Facial toners redundant?
Recently I've read an article in which facial toners were called a redundant step in the cleansing routine. They would not serve any purpose anymore and would be “old-fashioned". I disagree, and will explain why.
Particularly when you prefer wet facial cleansing (water has a pH of 7-8), your skin’s pH goes up and you may consider using a toner to bring it back to normal (~5) before using a moisturizer or serum. This also applies if you use an alkaline cleanser or micellar water. It is common that products which are suitable to be used around the eyes, like micellar water, are adapted to a more “eye-friendly” and less “skin friendly” pH of ~7. Skin prefers a pH of ~5. In my humble opinion, toners are a very important step in every a.m. and p.m. skin care regimen for both healthy and particularly problematic skin types. They refresh, remove left-over debris and make-up and moreover instantly rebalance skin’s pH value. A balanced pH value is the cornerstone for healthy skin. An optimal pH supports skin's microbiome (microflora or "ecosystem") and barrier function. Furthermore, the use of a toner usually helps the penetration and thus efficacy of your care product! Alternatively, you can use “chemical” exfoliating lotions or pads which contain AHA (glycol, citric and lactic acid), BHA (salicylic acid), PHA (gluconotactone), etcetera. Just be careful using them around the eyes or even avoid this area. Hope you enjoy healthy skin & take care. |
CategoriesAll Acne Ageing Aquatic Wrinkles Armpits Biostimulators Blue Light & HEVIS Cleansing CoQ10 Cosmetic Intolerance Syndrome Deodorant Dermaplaning Diabetes Dry Skin Evidence Based Skin Care Exfoliation Exosomes Eyes Face Or Feet? Facial Oils Fibroblast Fingertip Units Gendered Ageism Glycation Gua Sha Hair Removal Healthy Skin Heat Shock Proteins Hormesis Humidity Hyaluron Hyaluronidase Hypo-allergenic Indulging Jade Roller Licochalcone A Luxury Skin Care Lymphatic Vessel Ageing Malar Oedema Menopause Mitochondrial Dysfunction Mood Boosting Skin Care Neurocosmetics Ox Inflammageing PH Balance Skin Photo Biomodulation Polynucleotides Psoriasis Regenerative Treatments Review Safety Scarring Sensitive Skin Skin Care Regimen Skin Flooding Skin Hydration Skin Senescence Skip-Care Sleep Slugging Sunscreen Tanning Under Eye Bags Vitamin C Well Ageing Skin Care Wound Healing Wrinkles
Archives
April 2024
|


 RSS Feed
RSS Feed
